Specifying windows for behavioral healthcare projects

This article was originally published in February 2013. It has been refreshed and updated by Lisa May to further expand on the subject, including updates in industry standards and codes related to specifying windows for behavioral healthcare projects.
Whether replacing a dated, inefficient hospital or renovating an historic mental health institution, window selection is an important consideration in creating a modern, healing environment.
Behavioral healthcare facilities must minimize risks to patient safety, while maintaining a therapeutic environment. Windows provide daylighting and views to outside, helping create a more homelike and caring atmosphere for patients, while also contributing to staff health and well-being.
To ensure safety, behavioral healthcare facilities must meet comprehensive accreditation standards. A facility’s risk assessment depends on the patient population being served. Patient supervision and policies governing staff intercession, as well as control of patient access to various types of objects, are often site-specific variables. Risk also varies for areas within the building—seclusion rooms, bedrooms, and comfort spaces usually warrant consideration as higher-risk areas.
Selecting windows in patient-accessible areas calls for careful consideration. For behavioral healthcare applications, window products’ evaluation may include resistance to, or restriction of:
- escape attempts;
- patient access to unauthorized areas;
- attack to window components using blunt or sharp objects;
- tampering with, or disabling, locking devices;
- glazing infill exposure to flame or heat;
- chemical or bodily fluid resistance;
- laceration or self-harm by cutting;
- pica behavior (i.e. ingestion of components, materials, or coatings);
- abrasion, prying, or cutting of frame materials, glazing, or hardware;
- weaponization of parts that could be removed from window assemblies; and
- ligature, either intentional or accidental.
Due to site-specific variables, an adequate assessment can only be made through early consultation with the facilities management staff, security personnel, and treatment professionals.

Human impact testing
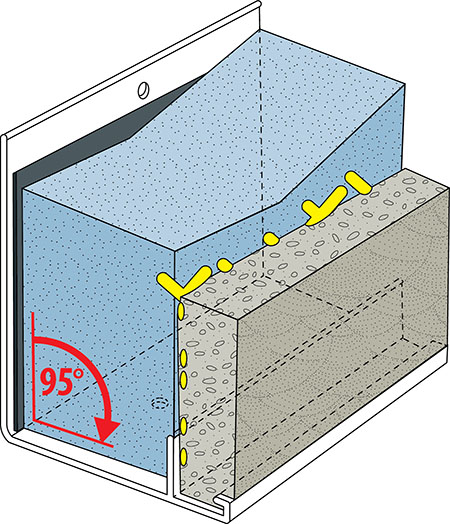
If a patient runs into the window, or if he or she strikes or throws an object against it, energy must be transferred sequentially through hardware, window frames, anchorage, and substrates. A human impact may impart as much as 2.7 kJ (2000 lb) of energy, based on the shoulder impact of a 90.7-kg (200-lb) person moving at 7.62 m (25 ft) per second.
This can require 12.7-mm (1⁄2-in.) thick polycarbonate or 11-mm (7⁄16-in.) tempered laminated glass for interior glazing. Standard windows fitted with safety glass or polycarbonate are seldom considered sufficient because interior glazing infill deflects on impact and may disengage from the standard window’s frame.
For a body hitting the window system, impact energy (W) can be calculated as:
W = ½ mv2
Where:
v = velocity at impact; and
m = mass of impact object
Using potential energy to calculate the energy imparted by a pendulum drop test, it can be calculated as:
W = wh
Where:
w = weight of impact object; and
h = vertical height the weight drops (not pendulum length).
When using either of these calculation methods, air resistance is considered negligible, and units must be kept consistent.
The need to validate the human impact aspect of the total window system’s security in the laboratory led to AAMA 501.8, Standard Test Method for Determination of Resistance to Human Impact of Window Systems Intended for Use in Behavioral Care Applications, a Fenestration and Glazing Industry Alliance (FGIA) document. It involves using a weighted impact device to apply a force simulating a patient running full-speed into a window. The test window complies when the window frame, glazing, hardware, and locking devices do not ‘fail,’ as defined by the performance requirements therein:
9.1. At the conclusion of testing the window system shall be deemed to pass the test if the following conditions are met:
The impact test load has not breeched or penetrated through the innermost glazing layer.
The innermost glazing remains held in place within the perimeter of the window frame.
Partial disengagement is allowed if meeting the requirements below:
- There is no damage to locking devices which would allow the window system to be opened in a manner not intended by the manufacturer.
- The window system does not disengage from any anchors securing the system within the opening.
- The window anchorage does not disengage from the substrate into which it was anchored during testing.
- The window hinges do not disengage to allow access to the exterior of the window system.
- No pieces may fall off the interior of the window such that they are accessible to the occupant(s).
- Frame joinery may be damaged, but must remain intact.
- Any tear or opening that develops in the interior glazing infill or at the perimeter of the interior glazing infill does not allow the passage of a 50 mm (2 in.) diameter sphere when a maximum force of 18 N (4.0 lb) is applied in line with the center of gravity of the sphere, which would allow egress or the passage of large objects, or allow access to the between-glass space. Partial penetration of the sphere through the system or into the between-glass space shall not be considered a failure.
- No de-lamination or separation of material greater than 322 mm2 (0.5 si) from the interior surface, immediately following the impact.
In certain occupancies, no delamination or discharge of material from the interior surface may be allowed. When this is deemed necessary, the specifier should so note in bid and contract documentation.

courtesy Apogee Architectural Metals
As with selection criteria, additional site-specific pass/fail criteria may apply to drop-tested behavioral windows. Depending on the furnishings and equipment accessible to the patients, simulation of physical attack with objects may be advisable. Exterior laminated glass should be used at windows at grade, courtyards, or porches with supervised patient access. Codes and standards vary widely by jurisdiction, so there should be consultation with onsite medical and security staff to determine appropriate resistance and necessary security.
It can be challenging to select products and materials that help create a pleasing environment, while enhancing the treatment process and maximizing safety. Selected resources offering guidance for material selection for inpatient behavioral units:
- Design Guide for Inpatient Mental Health & Residential Rehabilitation Treatment Program Facilities, published by the U.S. Department of Veterans Affairs (VA)
- The Design Guide for the Built Environment of Behavioral Health Facilities, distributed by the National Association of Psychiatric Health Systems (NAPHS)
- Design Guide of Behavioral Health Crisis Units, published by the Facility Guidelines Institute (FGI)
- Patient Safety Standards, Materials and Systems Guidelines, recommended by the New York State Office of Mental Health, developed in association with Architecture Plus of Troy, New York
These documents help examine the environmental aspects that can have a significant impact on patient safety and healing. The products they recommend have been evaluated to help lower patient risk.
Daylighting: enhance healing environments
“Views to the exterior that offer a positive distraction as well as a time reference can steady an individual experiencing discomfort, disorientation, and stress,” notes FGI’s Design Guide of Behavioral Health Crisis Units. In many new buildings, the design team attempts to maintain high visible light transmittance (VLT or VT) to ‘connect’ the occupants to the outside, provide views, and exploit natural daylighting. It is not only the amount of natural light that is important to building occupants, but also its quality, spectral composition, contrast, variability, and directionality.
Specifying tall windows helps maximize light penetration. Clerestories can be used to increase the effective height of transom lites without increasing window-to-wall ratio (WWR). Even relatively low WWR provides more than ample natural daylighting, when properly oriented and directed.
Within the programmatic limitations of a healthcare occupancy, natural daylighting is most energy-efficient if artificial lighting is automatically controlled. Photosensitive controllers and occupancy sensors can be used to dim or extinguish indoor lights when unnecessary. Artificial lighting accounts for about 40 percent of the energy used in a typical commercial building and generates at least three Watts of heat for each Watt of visible light.
Designers are encouraged to consider the concept of effective aperture (EA), the product of VT and WWR. Essentially, EA is the light-admitting potential of a glazing system, and determined by multiplying the WWR by the VLT. This can be useful when assessing the relationship between visible light and window size. One should start with an EA of about 0.3 on the north and south elevation, minimizing glazing on the east and west elevations whenever possible.
Unless “downward” view is important, vision glass should be eliminated below sill height to reduce solar heat gain that carries no useful daylight. Generally, the window area should be no different in naturally lit buildings than other conventionally lit ones.
In addition to sunlight and views of nature, high-performance window systems can assist with energy efficiency. Thermally broken frames with triple glazing, along with a broad selection of exterior glass options, provide enhanced energy performance and condensation resistance.

courtesy Apogee Architectural Metals
Integral between-glass blinds reduce solar heat gain, offer privacy control without the potential dangers of exposed cords, and minimize the need for maintenance. The tilting of the slats can be keyed for staff operation or to allow patient control with a low-profile ligature-resistant control knob. Raise-lower controls for between-glass blinds are usually limited to custodial access. Controlling raise-lower access allows for uniform blind placement vertically and a resulting consistent exterior appearance.
Many areas in hospitals are required to maintain high relative humidity (RH), as well as prescribed positive or negative internal pressure, for therapeutic reasons or contagion control. Condensation occurs on any interior surface falling below the dewpoint temperature (Tdp) of interior ambient air. Tdp is dependent on temperature and RH, as warm air can hold more moisture than cold air. Condensation can be unsightly, unsanitary, and damaging to adjacent building materials over long periods. For these reasons, condensation should be assessed for both frame and glass in applications where high humidity is maintained.
Finite element computer models and the condensation resistance factor (CRF) test results using AAMA 1503, Voluntary Test Method for Thermal Transmittance and Condensation Resistance of Windows, Doors, and Glazed Wall Sections, can be useful in comparing products or as a basis for performance specifications. The design professional should exercise caution when using these tools to predict or prevent condensation on installed products. Field condensation on interior surfaces is affected by many variables, including:
- component thermal performance;
- thermal mass of surrounding materials;
- interior trim coverage;
- air flow conditions;
- weather; and
- mechanical system design.
CRF applies only to pre-defined configurations under controlled and steady-state laboratory conditions; it assumes some condensation is acceptable under the severest of winter conditions.
Air infiltration through windows and walls is also important to total building energy performance. It not only takes “sensible” energy to heat or cool infiltrating air, but also may require “latent” energy to remove undesirable humidity. Air infiltration performance is usually considered separately from other thermal performance characteristics.

Photo by Mark Long/courtesy Apogee Architectural Metals
Facilitate ventilation and emergency egress
Although usually not required by code, some healthcare systems and government agencies, including the U.S. Department of Veterans Affairs (VA), recommend considering operable windows for their facilities. In the rare case of a fire, facilities with operable windows have the option of venting smoke and aiding egress.
Operable windows provide a backup for smoke evacuation in case of an engineered smoke control system failure and may alleviate the need for dangerous firefighter glass breakage to conduct emergency evacuation from the exterior. With operable units, custodians may quickly vent foul smells or noxious fumes. During normal operating conditions, concealed hinges and tamper-resistant locks prevent patients from compromising security by opening the window.
In hurricane-prone regions, wind-borne debris protection is also essential. Ensuring hospital windows stay intact during such an event keeps the building serviceable and protects occupants. These regions require large-missile-tested products at lower floors of healthcare facilities. In the event of an emergency, the laminated or polycarbonate security glazing will be practically impossible to break out—operable windows may be the preferred choice for firefighter access. Outside of hurricane-prone regions, healthcare facility managers are advised to consider their location’s likelihood of tornadoes or other natural disasters, as evacuation may be impossible.
Some healthcare facility professionals are surprised to learn about half of the states are susceptible to seismic activity. Large hospitals are “essential facilities,” classified as Occupancy Category IV by the American Society of Civil Engineers and Structural Institute/Structural Engineering Institute (ASCE/SEI) 7, Minimum Design Loads for Buildings and Other Structures. Guided by this standard, the International Building Code (IBC) includes detailed provisions to help hospitals not just withstand an earthquake, but also continue functioning during and after a seismic event.
To properly engineer windows and curtain walls to withstand earthquakes, parameters specific to the building and site must be considered. Glazing assemblies must elastically accommodate lateral seismic drift without glass breakage or losing weather resistance. Under inelastic movements, safety of occupants and passersby is critical. Additionally, inertial forces must be safely transferred to the building structure.
Early design coordination with adjacent wall system movement and anchorage provisions is essential for maintaining overall envelope integrity. The California Department of Health Care Access and Information (HCAI) helps ensure healthcare services remain available during and after major seismic events. Through strict adherence to HCAI administrative and technical requirements, project approvals are obtained in a timely manner.
Adapt for reuse
Renovations offer a healthcare facility manager a chance to enhance safety with improvements to the structure. For renovations or expansions, matching an existing structure’s window sightlines and symmetry can be challenging. Working closely with a glazing contractor and window manufacturer, healthcare facilities can achieve the desired aesthetic without compromising performance and safety. For major renovation projects, installation of in-situ samples is highly recommended.
The need for easy customization and durability has made aluminum an important material choice for historically influenced window replacement work. Applied muntin grids can help achieve a classic, multi-pane appearance. Environmentally responsible finishing service providers offer anodized and fluoropolymer painted aluminum as long-lasting options to match existing color schemes, without affecting indoor air quality (IAQ) by introducing volatile organic compounds (VOCs). Aging facilities may be returned to their original colors or updated after years of chalking, peeling, or expensive repainting.

Photos courtesy Oregon State Hospital/Apogee Architectural Metals
In cases when existing windows are weather-tight, and operation for ventilation is not required, the addition of high-quality, custodian-operable, interior-accessory windows can be a viable option, facilitating behavioral occupancy of structures originally intended for another use. With appropriate caution to avoid between-glass condensation and thermal stress breakage of existing glass, these economical add-on units improve control of sound, energy, air, and light, while leaving existing windows undisturbed.
The University of Minnesota’s Medical Center Fairview Behavioral Health Services renovated its facility for patient safety and energy efficiency. Privacy, security, and aesthetics were key considerations in selecting the window system. The new windows were configured with three lites per bay to echo the facility’s previous aesthetic. The specified windows are security-glazed with laminated glass for impact resistance, and a low-e coating for energy efficiency and condensation resistance. Even during Minneapolis’ freezing winter months, the windows help keep patients comfortable in their rooms.
Connect to the environment
Daylight and outside views, thermal and acoustic performance, and recycled composition of windows’ materials can aid buildings’ certification efforts under such programs as LEED. Since its inception in 2000, U.S. Green Building Council’s (USGBC’s) voluntary, consensus-based LEED rating system has emerged as the leading sustainable building “scorecard.”

Photo © Marilyn Ott-Close/courtesy Apogee Architectural Metals
Currently, LEED Building Design and Construction (BD+C) or LEED for Operations and Maintenance (O+M) both apply to healthcare facilities seeing certification. As of March 2025, there were 3,981 LEED‐certified and -registered healthcare projects worldwide, representing approximately 84 million m2 (904 million sf) of built space. Of these, 38 U.S. healthcare projects were LEED-certified in 2024, covering 6.3 million gross square feet. California had the most LEED-certified healthcare facilities in 2024 with 11 projects, followed by Texas with seven.
Other healthcare organizations may specify projects meet LEED criteria, but do not have to pursue certification. For example, the VA sustainability guidelines for facility construction and renovation projects require designing a project to meet LEED Silver certification or higher.
Environmentally responsible design and operation is a top-of-mind issue for anyone in architecture, construction, and real estate. Buildings represent about one-third of the energy consumption in the United States, along with the corresponding amount of greenhouse gas (GHG) emissions.
According to the National Academy of Medicine (NAM), “The health sector is a key contributor to climate change, generating 4.4 percent of carbon emissions globally and 8.5 percent of emissions in the United States.”
A question of economics?

Photo courtesy Apogee Architectural Metals
In 2011, an “Economics, Efficiency, Energy & Environment” survey was conducted by the Corporate Reality, Design, and Management Institute (CRDMI) in partnership with the Healthcare Council of the International Facilities Management Association (IFMA). Many of the 1251 respondents—architects, designers, engineers, hospital facilities managers, healthcare engineers, project managers, and contractors—underestimated the impact design and operations could have on a hospital’s financial health. The survey summary notes:
Given a 4 percent total margin, saving $1 in energy equals $25 in revenue, and for the average-sized hospital in the U.S. that translates to an additional $7.2 million in revenue.
Less than 15 percent of the 2011 survey respondents said they select products or equipment based on durability and expected lifecycle. Today, products’ material composition and longevity are increasingly under evaluation, including by programs such as the LEED and the International WELL Building Standard. Environmental Product Declarations (EPDs), Health Product Declarations (HPDs), Declare Label as Living Building Challenge Red List Free, and other supporting documentation assist specification and design professions with evaluation and selection.
By keeping any claims and representations focused on tested, third-party validated, performance parameters, as well as sound engineering judgment, manufacturers can present a credible case for their products’ support of sustainable design initiatives.
In Washington, D.C., Saint Elizabeths provides intensive, in-patient care for individuals with serious and persistent mental illness. (Under the aforementioned survey, only three percent of respondents from D.C. indicated sustainability features took precedence in the final selection of their last building project. Half of these participants also said LEED certification, or the U.S. Environmental Protection Agency’s [EPA’s] Energy Star for Buildings program would be the most important next step in pursuing sustainability goals.)
Established in 1852, Saint Elizabeths Hospital was the first large-scale, federally run hospital for people with mental illness. Its design incorporates numerous sustainable design elements emphasizing daylighting and external views. Patient safety and security remained a top priority. Windows were furnished with interior polycarbonate glazing for human impact resistance. The move into a new facility completed a transition from the historic, psychiatric institution into a modern, healing environment.
Conclusion
Whether building a new hospital, renovating existing spaces, or leveraging adaptive reuse of areas originally intended for another occupancy, window selection in areas accessible to psychiatric patients can be very challenging. Windows without jail-like bars or heavy security screens help create a more home-like and caring atmosphere with unrestricted views to the outside. At the same time, patient safety must remain the primary consideration.
Through development programs with state agencies and their architectural consulting partners, leading window manufacturers have designed psychiatric-grade fenestration systems answering this need.
Lisa May is the director of preconstruction and architectural services with Apogee Architectural Metals segment, providing technical assistance, sustainable design input, thermal modeling, detailing, and specification review to design professionals nationwide. She successfully completed Six Sigma training and the U.S. Green Building Council’s (USGBC’s) Leadership in Energy and Environmental Design (LEED) Green Associate accreditation. May instructs others in American Institute of Architects/Construction Specifications Institute (AIA/CSI)-approved continuing education programs addressing thermal and acoustical performance, and window and curtain wall selection. She can be contacted via email at lmay@apog.com.
Sign up for our weekly newsletter
Architectural materials and methods delivered right to your inbox
- CSI News & Notes: CSI’s impact earns official recognition; celebrate leaders, mentors, and innovators; and more
- CSI News and Notes: CSI spring certification exams open; scholarships available; and more
- CSI News & Notes: CSI MSR heading to San Diego; spring certification exams open; and more
- To Be Specific: Why CDT Should Be Your First Move
- CSI News & Notes: CSI Fellows share member benefits; and a New Year’s Resolution to keep
Products





Read the Latest Issue
